Metabolism
on-line - the virtual tutorial room
copyright © 2008 - 2015 David A Bender
Two boys with profound fasting hypoglycaemia and no ketone bodies
LF is an 18 month old boy. He is the first child of healthy non-consanguineous parents, delivered after a normal pregnancy. He was well until he had an episode of gastroenteritis, leading to diarrhoea and vomiting for several days, when he was admitted to hospital in a coma, with a blood glucose concentration of 1.0 mmol /L. There was no smell of acetone on his breath, and on testing his urine with a dipstick there were no detectable ketone bodies. He regained consciousness after an intravenous infusion of glucose.
Later during his stay in hospital he was fasted under close supervision, with blood samples taken at intervals over 18 hours, by which time he had become hypoglycaemic, and was given an intravenous infusion of glucose. The following results were obtained on analysis of blood samples taken during his fast (all in mmol /L):
LF |
control subjects |
||||
13 h fasting |
15 h fasting |
17 h fasting |
18 h fasting |
24 h fasting |
|
| glucose | 4.1 |
3.8 |
2.9 |
2.3 |
3.6 ± 0.4 |
| non-esterified fatty acids | 2.38 |
2.48 |
3.34 |
3.96 |
1.2 ± 0.2 |
| beta-hydroxybutyrate | 0.03 |
0.05 |
0.05 |
0.02 |
2.0 ± 0.2 |
| acetoacetate | nd |
nd |
nd |
nd |
1.0 ± 0.2 |
nd = not detectable
(From data reported by Morris AAM, et al, Pediatr Res 44:3
392-6, 1998)
What conclusions can you draw from these results?
The first impression is that LF appears to have a similar problem to TFP, who was unable to metabolism long-chain fatty acids, and therefore became profoundly hypoglycaemic on fasting (see the exercise on "Muscle weakness and hypoketotic coma on fasting"). However, in this case we have no evidence of muscle weakness. While it is possible the LF cannot oxidise fatty acids, it is also possible that he is able to oxidise them, but cannot synthesise ketone bodies from the resultant acetyl CoA.
In order to determine whether his problem was in the oxidation of fatty acids, or the synthesis of ketone bodies from acetyl CoA, fibroblasts were cultured and incubated with [3H]fatty acids. The results show nmol [3H]water released per hour per mg protein for two replicate assays on LF's fibroblasts and mean ± sd (and range in parentheses) for fibroblasts from 20 control subjects.
LF |
control subjects |
||
| [9,10-3H]oleate | long-chain, C18:1 n-9 | 3.7, 4.0 |
4.5 ± 0.8 (3.0 - 6.1) |
| [9,10-3H]myristate | medium chain, C14:0 | 6.0, 6.3 |
5.4 ± 1.0 (3.8 - 7.1) |
| [9,10-3H]palmitate | long chain, C16:0 | 5.8, 6.3 |
4.7 ± 0.9 (3.1 - 6.7) |
(From data reported by Morris AAM, et al, Pediatr Res 44:3 392-6, 1998)
What conclusions can you draw from these results?
There is obviously no problem with LF's ability to oxidise fatty acids, so the problem must lie in the synthesis of ketone bodies from acetyl CoA.
The pathway of ketone body synthesis is shown below
 :
:
.
 Hydroxymethylglutaryl
CoA (HMG CoA) is an intermediate in the catabolism of the amino acid leucine.
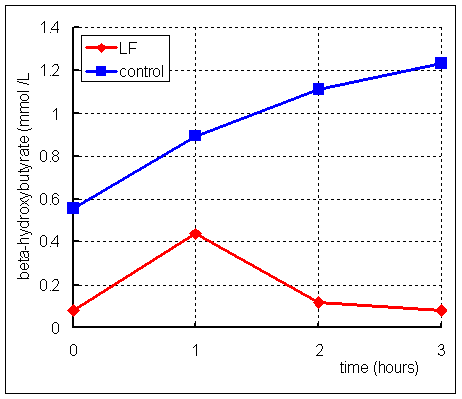
After an 11 hour fast, LF was given a dose of 200 mg /kg body weight leucine,
and blood samples were taken for measurement of beta-hydroxybutyrate. The results
are shown on the right:
Hydroxymethylglutaryl
CoA (HMG CoA) is an intermediate in the catabolism of the amino acid leucine.
After an 11 hour fast, LF was given a dose of 200 mg /kg body weight leucine,
and blood samples were taken for measurement of beta-hydroxybutyrate. The results
are shown on the right:
What conclusions can you draw from these results?
LF can obviously make beta-hydroxybutyrate from leucine, which means that he has adequate activity of HMG CoA lyase. Since he cannot make beta-hydroxybutyrate from fatty acids, this suggests that his problem is lack of either beta-ketothiolase or HMG CoA synthase. You do not know this at present, but beta-ketothiolase is also involved in the catabolism of ketone bodies, so it is most likely that he lacks HMG CoA synthase.