Metabolism
on-line - the virtual tutorial room
copyright © 2008 - 2014 David A Bender
Gout and hyperuricaemia - and anti-cancer drugs
There are links to a number of metabolic pathway diagrams in this exercise - in each case a .pdf file will open in a separate window - you may wish to print out the pathways, or just keep the Acrobat windows open to refer back to the diagrams.

Gout is an excruciatingly painful condition associated with the crystallisation of uric acid or its salts (urates) as gouty nodules (tophi) under the skin, in the synovial fluid of joints and in the renal tubules (nephrolithiasis). The condition is due to a concentration of uric acid in plasma greater than the limit of its solubility.
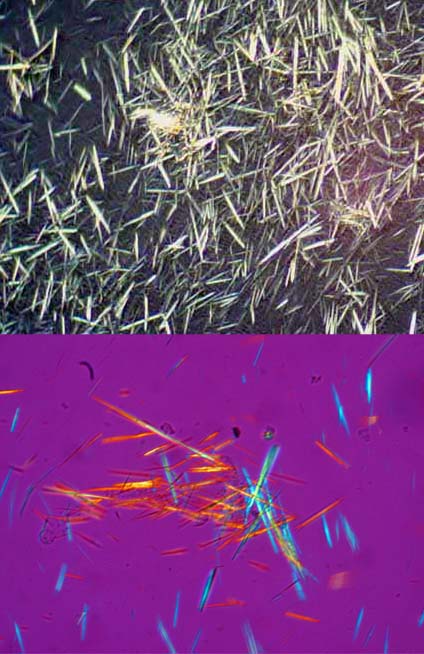 The micrographs on the right show uric acid crystals using polarised light.
The micrographs on the right show uric acid crystals using polarised light.
Uric acid is the end-product of the metabolism of the purine bases adenine and guanine; gout may be due to either impairment uric acid excretion or over-production of uric acid, associated with increased purine synthesis.
Rarely, a high dietary intake of purines (i.e. foods especially rich in RNA and DNA) may also be associated with the development of gout because of the considerably increased burden of purines to be metabolised.
An adult consuming an average diet excretes between 1.5 - 4.5 mmol of uric acid /day.
There is a familial tendency to develop gout, and there are significant differences in its prevalence among different ethnic groups, suggesting that, at least in some cases, there is a genetic factor.
Gout is mainly a disease affecting adult men; it is rare in pre-menopausal women, although post-menopausally women are at equal risk of gout as are men of the same age. Premenopausally, women have lower plasma concentrations of uric acid than do men.
plasma uric acid, mmol /L |
% with hyperuricaemia |
|
| men | 0.21 - 0.43 |
5 |
| women | 0.16 - 0.36 |
0.5 |
Plasma uric acid is more or less completely filtered by the glomerulus, but 98% of the uric acid in the glomerular filtrate is reabsorbed in the renal tubules. More distally, there is active secretion of uric acid into the lumen of the tubules. Much of the actively secreted urate is also reabsorbed. A number of compounds inhibit the active secretion of uric acid into the renal tubule, including the antituberculosis drug pyrazinamide and organic acids such as lactic acid, acetoacetate and beta-hydroxybutyrate.
You saw in the exercise on A hypoglycaemic adolescent with an enlarged liver and gout that Adam had persistent lactic acidaemia as a result of his glycogen storage disease.
Can you account for his development of gout at an early age?