Metabolism
on-line - the virtual tutorial room
copyright © 2008 - 2015 David A Bender
Was she murdered by insulin injection?
Mrs PI collapsed in a coma and was taken to the local hospital.
The results of blood tests were as follows:
Mrs PI |
reference range in fasting |
|
| glucose (mmol /L) | 1.2 |
3 - 5 |
| non-esterified fatty acids (µmol /L) | 190 |
700 - 900 |
| ketone bodies (µmol /L) | not detectable |
50 - 300 |
What do you think is the cause of Mrs PI's coma, and what is the likely cause?
She is profoundly hypoglycaemic. Like Ms CG in the exercise on Two diabetic patients in coma, this is probably the result of excessive insulin, either injected or the result of an insulin-secreting tumour of the pancreas (an insulinoma), since non-esterified fatty acids and ketone bodies are inappropriately low for someone who is so hypoglycaemic.
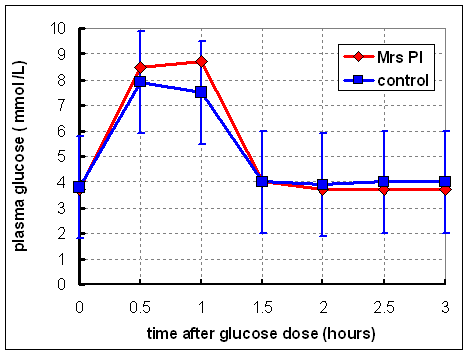 She was
kept in hospital for several days, appeared to be well, and was given an oral
glucose tolerance test (1 g of glucose /kg body weight). Plasma glucose was
measured over 3 hours. The results are shown on the right.
She was
kept in hospital for several days, appeared to be well, and was given an oral
glucose tolerance test (1 g of glucose /kg body weight). Plasma glucose was
measured over 3 hours. The results are shown on the right.
What conclusions can you draw from these results?
She is obviously not diabetic - at all times after the test dose of glucose her plasma glucose is within the norma range (shown by the error bars on the control curve).
Since she was now well, she returned home. On a number of occasions over the next few weeks she again collapsed in a coma, and was treated by glucose infusion, when she recovered consciousness.
She was known to drink heavily (several large gin-and-tonics each evening, and sometimes more). Her husband said that often she drank her pre-dinner gin-and-tonics, but then did not eat her meal.
How might drinking gin-and-tonic lead to hypoglycaemia?
The small amount of sugar in the tonic water causes insulin secretion, then the alcohol inhibits gluconeogenesis and glycogenolysis, so prolonging the hypoglycaemic action of the insulin. (This is how a small drink before dinner stimulates appetite, by causing mild hypoglycaemia).
One night she again fell into a coma, and this time died shortly after arriving at the hospital. A blood sample was taken before she died, and again showed that she was profoundly hypoglycaemic, with low non-esterified fatty acids and no detectable ketone bodies. Her blood alcohol was 75 mg /100 mL - just below the legal limit for driving.
Her plasma insulin was also measured, and was found to be extremely high - 2000 mU /L.
What conclusions can you draw from this information?
Her hypoglycaemia seems to have been caused by an abnormally high plasma concentration of insulin. If this is endogenous insulin then she must have an insulinoma (an insulin secreting tumour of the pancreas). However, the glucose tolerance test carried out aft she had been in hospital for several days was normal. If she had an insulinoma then you would expect to see a very much lower plasma concentration of glucose both before and after the oral dose.
It is, of course, possible that this was injected insulin, either self-injected or injected by someone else in a (successful) attempt to murder her, in which case suspicion might fall on her husband.
What we need is some way of differentiating between injected insulin (which these days is recombinant human insulin - i.e. insulin made in micro-organisms using the human insulin gene) and insulin secreted by her pancreas.
This is possible, but it means that we have to go back to studies of a then novel way of measuring insulin developed in the mid 1960s.
LC was born in 1967, at term, after an uneventful pregnancy.
 He was
a sickly infant, and did not grow well. On a number of occasions his mother
noted that he appeared drowsy, or even comatose, and said that there was a ‘chemical,
alcohol-like’ smell on his breath, and in his urine. The GP suspected
diabetes mellitus, and sent him to The Middlesex Hospital for a glucose tolerance
test (1 g of glucose / kg body weight after an overnight fast). The results
are shown in the diagram on the right.
He was
a sickly infant, and did not grow well. On a number of occasions his mother
noted that he appeared drowsy, or even comatose, and said that there was a ‘chemical,
alcohol-like’ smell on his breath, and in his urine. The GP suspected
diabetes mellitus, and sent him to The Middlesex Hospital for a glucose tolerance
test (1 g of glucose / kg body weight after an overnight fast). The results
are shown in the diagram on the right.
What conclusions can you draw from these results?
He is obviously diabetic, with a high fasting blood concentration of glucose and a very much higher than normal response to the oral dose of glucose.
Samples were also taken for measurement of insulin at zero time and 1 hour after the glucose load.
At this time a new method of measuring insulin by radio-immunoassay was being developed in research laboratories of The Middlesex Hospital, and therefore both this and the conventional biological assay were used.
 The
biological method of measuring insulin is by its ability to stimulate the uptake
and metabolism of glucose in muscle. Traditionally the diaphragm of a rat is
used for this biological assay, since it is easy to dissect out, and can be
cut into two halves of almost exactly the same weight. Both halves are incubated
with [14C]glucose, one with and one without the sample containing insulin, in
sealed "centre well" vials. At the end of the incubation an alkaline
solution is injected into the outer compartment top trap carbon dioxide, and
trichloroacetic acid is injected in to the inner well, containing the incubation
mixture, to stop the reaction and drive off carbon dioxide. This assay is relatively
tedious, and requires a rat for each sample to be analysed, as well as a number
of rats to calibrate the assay against known amounts of insulin.
The
biological method of measuring insulin is by its ability to stimulate the uptake
and metabolism of glucose in muscle. Traditionally the diaphragm of a rat is
used for this biological assay, since it is easy to dissect out, and can be
cut into two halves of almost exactly the same weight. Both halves are incubated
with [14C]glucose, one with and one without the sample containing insulin, in
sealed "centre well" vials. At the end of the incubation an alkaline
solution is injected into the outer compartment top trap carbon dioxide, and
trichloroacetic acid is injected in to the inner well, containing the incubation
mixture, to stop the reaction and drive off carbon dioxide. This assay is relatively
tedious, and requires a rat for each sample to be analysed, as well as a number
of rats to calibrate the assay against known amounts of insulin.
The then newly developed method of measuring insulin is by its ability to bind to anti-insulin antibodies, in competition with radioactively labelled insulin - this is radio-immunoassay, and is generally preferred because it is possible to assay a large number of samples at the same time. The antibody recognises, and binds to, the surface of the tertiary structure of the protein.
Why do you think that both assay methods were used at this time?
The radio-immunoassay was new, and had not yet been demonstrated to be as good as the biological assay. The assays were performed in the research laboratory as part of the process of validating the new assay method.
The results of the insulin assay were as follows (in mU of insulin /L):
biological assay |
radio-immunoassay |
|||
fasting |
1 h after glucose |
fasting |
1 h after glucose |
|
| LC | 0.8 |
5 |
10 |
50 |
| control subjects | 6.2 ± 2 |
40 ± 11 |
6.1 ± 2 |
40 ± 11 |
Why do you think insulin is measured in units (here mU /L)?
This goes back to the early days of insulin, when it was not possible to measure it chemically, and its molecular mass was unknown. The only way of measuring insulin (until the development of radio-immunoassay) was by its biological activity.
 The unit
of insulin was originally that amount that would reduce the blood glucose concentration
of a 1 kg rabbit by a given amount over 1 hour. Later work recalibrated the
unit in terms of the effect on the metabolism of glucose by rat diaphragm incubated in vitro - originally measuring the volume of carbon dioxide released
by manometry, then later by the release of [14C]carbon dioxide from [14C]glucose.
The unit
of insulin was originally that amount that would reduce the blood glucose concentration
of a 1 kg rabbit by a given amount over 1 hour. Later work recalibrated the
unit in terms of the effect on the metabolism of glucose by rat diaphragm incubated in vitro - originally measuring the volume of carbon dioxide released
by manometry, then later by the release of [14C]carbon dioxide from [14C]glucose.
Insulin syringes are calibrated in units, not volume.